Archive for the ‘Stem Cell Therapy’ Category
LIVING WITH BACK PAIN
In most instances, individuals with low back pain will improve over a two- to six-week period. The goal is to minimize recurrences and, while being in good physical condition does not prevent all back pain episodes, it will make the resolution of those episodes easier. If you smoke, stop. Smoking is a predisposing factor for back pain. If you are overweight, get into shape. Obesity does not cause back pain, but it does make it harder to heal. (No particular diet is known to prevent episodes of low back pain.) Bottom line, pay attention to your body and exercise, eat right and maintain a healthy life style.
POINTS TO REMEMBER
- Low back pain is a common problem and rarely associated with a severe illness.
- The vast majority of individuals heal back pain by remaining active and taking pain-relieving drugs.
- About 50 percent of individuals are healed in a week or two; over 90 percent are resolved in eight weeks.
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us

Share this:

Dallas Spine Pain Center, Spine Pain Help Dallas, Dallas Spine Pain Doctors
If you are looking for a specialist in spine surgery, Dallas may be your next destination. BecomePainFree.com’s Dallas office provides:
- A free MRI or CT scan evaluation by medical staff
- Partner physicians board-certified in interventional pain management
- Free educational back pain seminars
- One of the top surgical facilities in the country
Free MRI or CT scan evaluation. Have you tried conservative therapies for your chronic back pain, and wonder if a medical procedure is the next best step? Allow our staff to evaluate your medical case. Our physicians will provide the most conservative recommendation deemed appropriate for your special case.
Free medical referral service. If you choose, your assigned patient coordinator will handle the logistics for any medical procedure recommended by one of our physicians.
Board-certified physicians. Our Dallas-based specialists collectively provide expertise in neurosurgery and interventional pain management, and provide a range of procedures, from epidural steroid injections to spinal fusion. They are unique providers of the BecomePainFree.com procedure.
Free back pain seminar. BecomePainFree.com’s Dallas office provides regular educational seminars so chronic pain sufferers can learn about the BecomePainFree.com procedure and talk directly to someone who can answer all of their questions.
Surgical facility. Victory Medical Center in Plano, TX is one of the newest surgical facilities in Dallas-Fort Worth.
Located in the center of the United States, the Dallas laser spine center also provides a convenient option for chronic back pain sufferers across the country – just a short plane-ride away. BecomePainFree.com’s Dallas office has partnered with the Hyatt Place, for traveling patients.
The BecomePainFree.com headquarters is also in Dallas TX. So when you visit, make sure to say hello to the patient coordinator and insurance teams, who strive to help patients like you find a solution for their pain.
Address:
13601 Preston Road, Suite E575
Dallas, TX 75240
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us
About us: BecomePainFree.com provides patient advocacy for spine pain sufferers. Patient care may be described as a table with patients on one side looking for a solution, and physicians on the other side providing a service; since BecomePainFree.com does not practice medicine, it is uniquely positioned on the patient’s side of the table, providing a compass to navigate the often confusing world of spine surgery and interventional pain management.
https://www.becomepainfree.com/

Dallas skyline (Photo credit: dherrera_96)
Share this:

San Antonio Spine Surgeon, San Antonio Back Doctor, Mayo Clinic Trained Spine Surgeon, Bexar County Orthopedic Surgeon
Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us
Share this:

Spine Surgeon Dallas, Mayo Clinic Trained Spine Surgeon, Back Doctor, Spine Pain Doctor
https://www.becomepainfree.com/
Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us
Share this:

Stem Cells for Spine Surgery: 7 Points
Written by Laura Miller | May 23, 2012
Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us
How we got here
Dr. Hynes was one of the many spine surgeons who participated in Medtronic’s original trials for BMP-2 in the 1990’s. While scientists have known about the ability of stem cells and BMP to generate bone for several years, Medtronic was the first company to develop a safe and effective molecule to stimulate cell growth. After completing the pre-market approval trials, the Food and Drug Administration granted approval for the BMP-2 product, Infuse, in 2002 for creating fusion in the Lumbar Spine placed through an anterior approach in a LT cage.
“In the original study, I experienced 100 percent of enrolled patients in my Practice achieving bone growth when combining BMP with the local cells that were already there,” says Dr. Hynes. “Local ‘stem cells’ respond to BMP and become activated thereby creating bone. When I saw it worked in 100 percent of my enrolled patients, I was a true believer. I have used it in my practice since the study and FDA approval going back greater than 10 years.”
What has changed is our ability to concentrate stem cells; Dr. Hynes harvests the stem cells from the iliac crest to combine with the BMP. It takes less than five minutes for his physician’s assistant to harvest the cells, which are spun in a centrifuge while he begins the operation. After 10-15 minutes, the cells are ready and Dr. Hynes adds a small amount to the surgical field along with the BMP. The collagen sponge is placed within an interbody LT cage to keep the material from migrating.
“This has been an effective Bone Graft method and it has been an advantage for my patients who can avoid Iliac Bone Graft surgery and Donor Bone issues and cost,” says Dr. Hynes. “It doesn’t add to my usual procedure time. It does add a small cost, but I find it’s worth the value proposition.”
Since its inception and release, surgeons have been experimenting with its use in several different capacities, on- and off-label. However, articles published in The Spine Journal in July 2011 suggest complication rates may be higher than the original studies reported. Several physicians have reported positive and negative events based on individual practice date, and further research into its use will be necessary going forward. As with all products, on label and off label use is routine practice and common place. When used correctly, minimal side effects of swelling, seroma and osteolysis occur.
What the research says
There have been several clinical studies and basic science research projects published in professional journals discussing the efficacy of using BMP with local stem cells to enhance fusion. However, research on the impact of increasing the number of stem cells is still lacking. Dr. Hynes’ current clinical work focuses on whether there is a better chance of achieving fusion with a higher concentration of stem cells.
He harvests stem cells from the iliac crest, percutaneously and painlessly, or vertebral body and extract about 60-80 ccs of blood. The desired stem cells are concentrated to a few ccs with centrifugation and has about a 50,000 cell count per “Spine Smith research data.”
“We already know the mechanism by which BMP-2 activates stem cells. The stem cells are already very effective,” says Dr. Hynes. “If we add to the population of stem cells that are already there that are available to regenerate new bone, it could make the procedure even better. Anecdotally, I have a high fusion rate for my spine patient population even before adding the extra concentration of stem cells. With the additional stem cells, I hope to achieve fusion at almost any level no matter how many levels are needed such as in degenerative scoliosis. In osteoporosis and aging spine patients, this has been extremely beneficial when compared to poor iliac crest from bone harvest.
Dr. Hynes’ ethereal practice goal is to someday be able to “guarantee” that they will achieve fusion for every patient who undergoes surgery. This means stabilization. However, fusion does not guarantee “success” of the surgery but increases odds of the surgical success. At this point, he is close, with approximately a 95 percent fusion rate. “What I want to do before I retire is to be able to guarantee a fusion,” he says. “I can’t guarantee pain relief or other clinical outcomes, but I want to be able to confidently guarantee the fusion or stabilization component.”
Options for harvesting stem cells
There are several bone graft options spine surgeons can choose from to achieve a fusion, and in the wake of recent controversies some surgeons are looking for an alternative to using BMP. Surgeons can go back to the traditional fusion method – the iliac crest – or using an allograft. Dr. Hynes says harvesting bone from the iliac crest can leave 30 percent of patients in more pain and add significant surgical time in the OR with increased blood loss. Allografts also have downsides, including graft consistency, quality, processing issues and less potential to achieve fusion than iliac crest or autogenous grafting methods.
“The bone for allografts may not be prepared correctly,” says Dr. Hynes. “We don’t always know the quality or consistency of the allograft compared to the patient’s natural bone. If I’m putting a piece of bone in patients, it’s better if it comes from their own bodies. That way, you can’t tell the difference between the bone you grow and the natural bone. (What we are doing is creating a nice bone graft that balances the biomechanics of the fusion construct better than the allograft.)”
In some cases, the allograft bone could migrate or fracture or reabsorb after the procedure, which can cause significant pain and complications, often resulting in revision procedures. By using the combination of BMP and stem cells in an interbody device, Dr. Hynes is able to avoid most of those complications because the cells are attracted to the BMP, which is restrained in the cage.
Patients should have the final say – “Informed Consent”!
Like many surgeons, Dr. Hynes describes the different fusion options to his patients and allows them to choose which procedure they feel most comfortable with. He discusses the pros and cons of each technique, including the most recent concerns about BMP, as well as his personal outcomes. He says patients often choose BMP combined with stem cells because they like the idea of regenerating their own bone naturally, avoiding the extra surgery and potential pain of iliac crest bone grafts and decreased potential or effect of donor allograft bone.
“The psychology of healing is part of this,” says Dr. Hynes. “Patients understand the procedure and like the idea of using their own cells as healing factors. People are very positive about that process because they feel like they are doing something natural instead of synthetic. Healing and surgery isn’t just biomechanics and science; it’s psychological as well. Successful outcomes of surgery depend on subjective relief as well as objective factors.”
In his practice, Dr. Hynes says a significant number of his patients chose the BMP and stem cell combination with given the option. However, when the patients choose a different option, he performs the other procedures as well. “It’s our duty to give patients their choice,” he says. “I’m not always smart enough to know what the best choice is for any one individual, but I’ve practiced many years and learned that if you take time to educate patients to all the reasonable options, they will make good decisions and take responsibility for them.”
Deciphering the complications
While Dr. Hynes hasn’t experienced significant complications among his patients, it’s clear that other surgeons have reported complications when they perform spinal fusions using BMPs. One reason for the discrepancy could be the dosage; well-documented evidence suggests that a higher dosage of BMP could cause swelling complications when used in the cervical spine. By using low doses of BMP and a pre and post-surgical protocol, swelling is completely avoidable in the cervical spine. Another factor is the surgical approach; Dr. Hynes says retrograde ejaculation (“RE”) – one of the severe complications mentioned in the studies this past summer – is a complication risk of any anterior spine surgery and not related to use of BMP. “I have performed thousands of anterior procedures before and after approval of BMP for anterior lumbar surgery and I find no difference in RE noted in my patients.”
“Every spine surgeon knows RE is a risk during anterior procedures and it usually will reverse on its own,” says Dr. Hynes. “RE occurs in an extremely low frequency. RE occurs because of disruption ‘surgically’ of small nerves to a sphincterine the bladder. BMP does not cause this effect, but the use of the electrocautery tool, during surgery, likely does. Use a small dose of BMP and a cage as well.”
In his practice, Dr. Hynes has never experienced a critical airway complication using cervical BMP. In early years, too high a dose would lead to swelling but not airway compromise which more commonly occurs with hematoma or blood clot, says Dr. Hynes. Papers published in The Spine Journal also mention cancer as an associated complication, which is something he hasn’t necessarily noted either. “I haven’t seen a rash of cancer in my patients, but I haven’t been surveying for it either,” he says.
He is currently going through his patient base to determine whether he can detect any cancer cases that could be associated with the procedure.
Whether to use BMPs
As surgeons report different findings based on their individual practice data, many of the studies and discrepancies have been reported in the media. However, full understanding of these complex issues is often lost in news reports. “I hate to see some of the surgeons and journals duking it out in the media,” says Dr. Hynes. “That isn’t the place to argue over the efficacy of stem cells and BMPs. We have to do it in the meetings where people understand the context. To lay this out in the newspapers exacerbates political agendas and confuses our patients. We need to speak honestly with each other about this at professional and scientific meetings, not in the press.”
This controversy isn’t the first time new spinal technology and procedures have been under attack. For a period of time, pedicle screws – which are a standard of care now – were under the microscope because complications were reported. In some instances, surgeons were sued and restricted from use at their hospitals for their alleged unfavorable outcomes. Now pedicle screws are the mainstay of spinal fusion procedures.
“At the time, there was only approval that pedicle screws could be used on single-level surgeries,” says Dr. Hynes. “Now we use them at multi-levels. The pedicle screws ultimately won the day, but with public stimulation ‘in the news’ in the early 1990s, we almost lost the ability to use them. This was a public attack on the advent of a new fusion technology, and now we are seeing similar phenomenon’s with BMP and other medical products.”
Covering the cost of BMP
In some cases, surgeons may have a difficult time receiving reimbursement for BMP products because they were more expensive in the past. Dr. Hynes and his colleagues have worked with hospitals and surgery centers to cover the cost in both out-of-network and in-network contracts. In some cases, patients are willing to cover the cost of using stem cells with BMP. Due to the success and demand, the cost has now become competitive considering operative costs of iliac bone surgery or allograft. “The increased volume of use and effectiveness has caused a dramatic decrease in cost,” says Dr. Hynes.
“I see patients from out of the Country and they are usually cash pay patients,” says Dr. Hynes. “We have to line item every part of the procedure to show the actual cost and there is almost no increased cost for the use of low concentrated BMP compared to iliac bone grafts or allograft when taking OR time, surgeon’s time and other OR costs into consideration.”
Fortunately, the hospitals in Dr. Hynes’ community allowed him to use BMP and conduct the clinical studies there. “We have more experience in our community with the benefits of this technology because we started so early,” he says. “Our surgeries are very efficient and our operative time is less because of our long-term experience with the procedure using stem cells and BMP.”
However, in some cases Dr. Hynes has made sacrifices to mitigate these costs. “I think about what I could live without and forego those expenses for stem cells and BMP,” he says. “I might use less expensive blades or a new set of tools for the next year. I might continue to use my old led apron or do surgery without a super drape. I’m there to give patients a better outcome and I want to make sure they have the opportunity to have the stem cells.”
More Articles on Spine Surgeons:
8 Spine Surgeons on the Future of Spinal Fusions
6 Spine Surgeons on How Young Surgeons Can Position Themselves for Success in the Future
What Percentage of Your Spine Practice is Medicare Patients?
Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us
Share this:

BecomePainFree.com Treats
- https://www.becomepainfree.com/
Herniated discs - Pinched nerves
- Degenerative spine disease
- Spinal stenosis
- Spondylolisthesis (slipped spine)
- Scoliosis (deformity)
- Low back pain / neck pain
- Spine trauma
- Spine infection
- Osteoporotic fractures
- Spine and spinal cord tumors
- Peripheral nerve injury
- Chiari malformation
- Cavernous malformation
- Vascular malformation
Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us
Share this:

Central Cord Syndrome
Central Cord Syndrome (CCS) is an incomplete injury to the cervical cord resulting in more extensive motor weakness in the upper extremities than the lower extremities. The mechanism of injury occurs from a hyperextension injury with pre-existent osteophytic (abnormal bony outgrowth) spurs, without damage to the vertebral column.

Mechanism and Causes of Injury
CCS occurs typically in patients with hyperextension injuries where the spinal cord is squeezed or pinched between anterior cervical spondylotic bone spurs and the posterior intraspinal canal ligament, the ligamentum flavum. The ligamentum flavum is a strong ligament that connects the laminae of the vertebrae. It serves to protect the neural elements and the spinal cord and stabilize the spine so that excessive motion between the vertebral bodies does not occur.
The injury occurs as a result of anterior and posterior compression of the spinal cord, leading to edema, hemorrhage or ischemia to the central portion of the spinal cord. The site of most injuries is in the mid-to-lower cervical cord. Due to the anatomical lamination of the corticospinal tract with the arm fibers medially, and the leg fibers laterally, the arms are affected more so than the legs, resulting in a disproportionate motor impairment.
Symptoms
Patients are typically left with motor weakness of the upper extremities and lesser involvement of the lower extremities. A varying degree of sensory loss below the level of the lesion and bladder symptoms (urinary retention) may both occur.
Incidence
This syndrome more commonly affects patients age 50 and older who have sustained a cervical hyperextension injury.
CCS may occur in patients of any age and is seen in athletes who present with not only hyperextension injuries to their neck but associated ruptured disc(s) with anterior cord compression.
CCS affects males more frequently than females.
Diagnosis
Evaluation of the patient includes a complete history, a thorough neurological exam, MRI and CT of the cervical spine, and cervical spine x-rays including supervised flexion and extension x-rays.
- Magnetic resonance imaging (MRI): A diagnostic test that produces three-dimensional images of body structures using powerful magnets and computer technology; can show direct evidence of spinal cord impingement from bone, disc, or hematoma.
- Computed tomography scan (CT or CAT scan): A diagnostic image created after a computer reads x-rays; can show the shape and size of the spinal canal, its contents, and the structures around it.
- X-ray: Application of radiation to produce a film or picture of a part of the body can show the structure of the vertebrae and the outline of the joints. X-rays of the spine delineate fractures and dislocations, as well as the degree and extent of spondylitic changes. Flexion/extension views assist in evaluation of ligamentous stability.
Surgical Treatment
Acute surgical intervention is not usually necessary unless there is significant cord compression. Prior to the CT-MRI era, surgical intervention was thought to be more harmful because of the risk of injuring a swollen cervical cord and worsening the deficit. However, with advanced imaging technology such as CT and MRI, patients with compression of the spinal cord secondary to traumatic herniated discs and other lesions can be quickly diagnosed and surgically decompressed. In cases with anterior bony ridges and spinal canal narrowing secondary to ligamentous thickening and or stenosis, acute surgery is usually not performed until the patient has made maximum recovery. Reassessment at that time may lead to surgery depending on the underlying cause. If there is significant motor weakness after a period of recovery, or neurological deterioration or spinal instability, then surgical intervention may be considered.
Nonsurgical Treatment
Nonsurgical treatment consists of immobilization of the neck with a cervical orthosis, steroids unless contraindicated, and rehabilitation with physical and occupational therapy.
Outcome
Many patients with CCS make spontaneous recovery of motor function while others experience considerable recovery in the first six weeks post injury.
If the underlying cause is edema, recovery may occur relatively soon after an initial phase of motor paralysis or pareses. Leg function usually returns first, followed by bladder control and then arm function. Hand movement and finger dexterity improves last. If the central lesion is caused by hemorrhage or ischemia, then recovery is less likely and the prognosis is more devastating.
The prognosis for CCS in younger patients is favorable. Within a short time, a majority of younger patients recover and regain the ability to ambulate and perform daily living activities. However, in elderly patients the prognosis is not as favorable, with or without surgical intervention.
Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us
Share this:

Regenerative Medicine
Administering undifferentiated stem cells to an injured disc has made adult stem cell regenerative medicine in spine a reality. Adult stem cell regenerative medicine holds the promise of stabilizing or even reversing the degenerative changes associated with aging or following traumatic injury. Current clinical use of stem cells is very limited, in part by the cumbersome approval process. The use of concentrated bone marrow aspirate (BMC) as a “stem cell” preparation is currently the simplest and safest way of utilizing the regenerative potential for mesenchymal stem cells (MSCs) to promote tissue regeneration. In fact, stem cells concentrated from bone marrow have been shown to stimulate the formation of bone, cartilage, ligament and tendon, and dermal tissues.
Conservative treatment options for lumbar and cervical pain associated with discogenic disc disease (Pfirrmann Grades 3-6) are limited. Treatment options include pain medication, steroids, physical therapy, and chiropractic care. Reversal of disc pathology has not been achieved with current available treatment modalities. Failure of these nonoperative treatments may leave surgical intervention as a treatment option.
The goal of utilizing MSCs is to not only potentially provide pain relief from the painful degenerative disc, but to reverse the degenerative process. There are three methods for placing MSCs into the painful nucleus pulposus.
The use of allogeneic mesenchymal precursor cells (MPCs) is currently being evaluated as a part of an FDA Phase I clinical trial. Extracted from donors and expanded in number by tissue culture, this process isolates and grows the stem cells into pure MPCs which are injected into the nucleus pulposus. This technology does not have FDA approval.
Utilizing expanded, autologous MSCs for injection into the painful disc is the second method. Federal regulations require the approval of an Investigational New Drug application supported by prospective, randomized clinical trials for the use of expanded autologous MSCs. The FDA has not approved this technology.
The third method involves autologous point of care therapy. This technology does not require FDA approval. The patient’s own MSCs are directly injected into the nucleus pulposus of the symptomatic degenerated disc(s) using standardized two needle discography technique. This requires fluoroscopic visualization and 2-3cc of MSCs are slowly injected into the symptomatic nucleus pulposus.
There have been no complications associated with the iliac crest aspiration or disc injection. Thus far no patient in the study has undergone spine surgery following treatment. Results obtained with this technique suggest its potential clinical efficacy in the treatment of moderate to severe degenerative disc disease. These results require verification with longer follow-up and randomized prospective studies.
For more information regarding treatment options please visit our websites at http://www.becomepainfree.com
Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us

Share this:

Adult Stem Cell Therapy to Treat Back Pain, Stem Cell, Spine Stem Cells, Stem Cell Treatment
Adult Stem Cell Therapy that doesn’t require FDA approval to treat lumbar and cervical spine conditions resulting from injury or aging, and is also involved with an FDA clinical trial investigating the use of Adult Stem Cells.
Stem Cell
These stem cells are autologous – they are taken from an adult patient and returned to that same patient in a concentrated form to the damaged area in a 30-minute procedure. This type of adult stem cell therapy does not require FDA approval to administer.
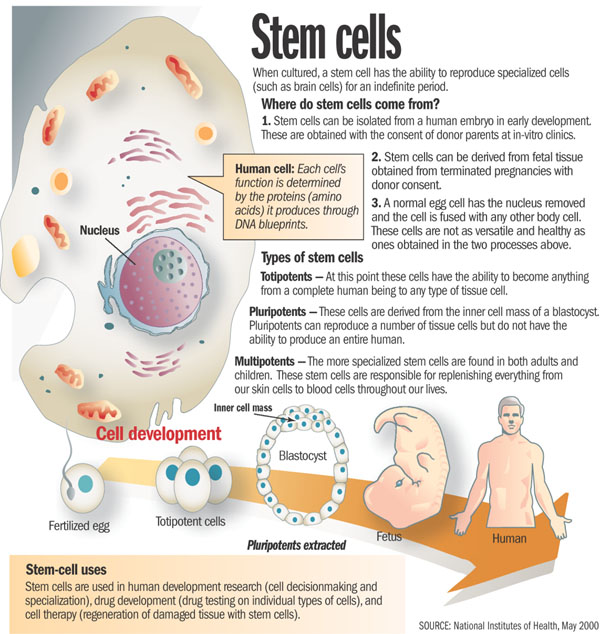
When it comes to stem cells, there is often a lot of mystique surrounding them. We hear from the media that we can create a human being out of a bundle of cells, which is not necessarily true. We also tend to look at embryonic stem cells as being the only type of stem cell. With these types of embryonic stem cells, one idea is to be able to create a liver or kidney in a Petri dish, which is not controllable or feasible at this point, and the work being done by the BecomePainFree.com medical group.
When we look at stem cell types, we have embryonic stem cells on one hand and adult stem cells on the other. The characteristics of each of these are not like other cells. For instance, a liver cell can divide but it will only ever be a liver cell. These stem cells, both embryonic and adult, can turn into different types of cells. The embryonic stem cells can really turn into any cell type, but adult stem cells are limited as far as the cells they can turn into. This depends upon environment or niche and what they are already programmed to become. A lot of people think there is a lot of promise with embryonic stem cells and there is, although we are not quite there yet.
We are still at the forefront of stem cell technology and embryonic stem cells in particular. With those cells, we do not have the ability to control what types of tissue they turn into. For example, we could be trying to manipulate these cells to turn into kidneys, but they might start to develop as pancreatic cells, which is troublesome. Another key with all stem cells is that they can proliferate quite a bit, usually at a higher rate than just a regular somatic cell. Although this sounds good at first glance, the issue with this, particularly with embryonic stem cells, is we cannot control that division. Hence, these cells can keep going and going without dying. In the normal bodily process, cells are programmed to die after a certain time, but these embryonic stem cells can evade that action and continue dividing, which takes on the characteristic of cancer cells. In some animal studies, an issue that keeps arising is development of tumors in some of these animals. It is difficult to predict if tumors are going to form when using some sort of embryonic stem cell treatment. This is still a scary area through which we are still trying to navigate.
However, the focus of the BecomePainFree.com medical group is on adult mesenchymal stem cells. On the whole, the media does not give a lot of attention to these kinds of stem cells, as using them avoids any kind of ethical or controversial issues. There is a great amount of research being done on adult mesenchymal stem cells, however, because they are very powerful.
First off, we can control what cell type they turn into much more easily. For example, the treatment used by the BecomePainFree.com medical group focuses on Mesenchymal precursor cells (MPC). Mesenchymal means these cells are not going to turn into any kind of blood product such as a red blood cell or white blood cell, although they are derived from bone marrow. The fact that they are precursor cells means these MPCs are only going to differentiate into one of a few cell types. They are either going to become bone cells, i.e., osteoblasts, or chondrocytes, i.e., cartilaginous tissue such that we see in intervertebral discs and joints, etc. All of that really depends on the environment in which we place these adult stem cells where it is well suited to do this. For example, we can inject these MPCs into a bone fracture, and because the cells are surrounded by bone tissue, these cells will receive signals from the surrounding cells that tell them to turn into bone. However, the cells we use will be injected into a disc or joint, and the cells composing the disc and joint tissue will signal the stem cells to develop into similar tissue. Again, there is no chance of any sort of pancreatic cell or nerve cell type spontaneously forming because we are using certain adult stem cell types, which are limited and cannot turn into anything like that. In addition, as the tissue surrounding the disc and joint is relatively avascular, there is not really any worry of these cells migrating through the blood stream to somewhere else in the body and causing any sort of problem. As far as the proliferation issue with embryonic stem cells, we have not seen this issue with adult stem cells in terms of dividing exponentially without ceasing. There is almost a preset limit to how many times these adult stem cells will divide.
Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us https://www.becomepainfree.com/
Share this:

Mayo Clinic, Spine Surgeon, Mayo Clinic Back Surgeon, Mayo Clinic Pain, Mayo Clinic Fellowship Trained Surgeon, Mayo Clinic Doctor, Mayo Clinic Back pain
We have two spine surgeons in our group and one on the way from the world famous Mayo Clinic. These Mayo Clinic surgeons are some of the best in the United States of America both of these Mayo Clinic trained doctors work in Texas. Dallas, Fort Worth, San Antonio we ave you covered with Mayo Clinic trained spine surgeons. Here is the information on these doctors below.Check out our website at https://www.becomepainfree.com/
Call Us: (214) 396-3647 | (888) 373-3720
Fax #: (888)238-9155 | E-mail Us
Steven J. Cyr, M.D., FAAOS
Mayo Clinic Trained Spine Physician

Steven J. Cyr, M.D., is a Board Certified Orthopaedic Surgeon who received extensive training to specialize in the delicate science of Spine Surgery. Anyone who knows Dr. Cyr well will tell you that he is a man driven for quality and excellence. His high standards can be seen throughout his educational process and career.
He received top honors at Southwest Texas State University by graduating Summa Cum Laude and Valedictorian with a Bachelor of Science in Biology. In addition to rigorous academics, he was also a member of the Bobcat football team during his three years at SWTSU.
Dr. Cyr gained early acceptance into medical school and earned his MD from the University of Texas Health Science Center in San Antonio. He then began his service to the United States Air Force with a transitional internship at Wilford Hall Medical Center. He served the air force community as a flight surgeon for two years before beginning residency training in orthopaedic surgery at Wilford Hall.
Following residency, Dr. Cyr was honored to be chosen from among the country’s top residents as the only fellow for the highly competitive and prestigious spine fellowship at the Mayo Clinic in Minnesota. This training program has ranked number one for orthopaedic and neurosurgical training programs in America for the last 20 years. Mayo combines these two fields, giving their surgeons an understanding of nerve and spine function unparalleled in most other programs.
Upon completion of his fellowship, Dr. Cyr and his family moved back to San Antonio, where he served the military population as the Chief of Air Force Spine Surgery and Spine Surgery Consultant to the Surgeon General of the Air Force. For six years, Dr. Cyr taught future air force orthopaedic surgeons in residency at Wilford Hall and has twice served our war wounded in Iraq at the Air Force Theater Hospital in Balad.
He has brought innovative techniques to the military and was the first to perform the total disc replacement procedure as well as endoscopic spinal surgery. He specializes in complicated spine issues and has gained notoriety for successful repairs of failed surgeries on patients from numerous other states and around the world. Dr. Cyr’s expertise and skills are now available to civilian patients at the Orthopaedic and Spine Institute, where his passion for excellence and quality keep him at the leading edge of spine surgery.
Mayo Clinic Trained Spine Physician
Dr. Venkat Sethuraman M.D.

Mayo Fellowship Trained Board-Certified Spine Surgeon
Minimally Invasive Spine Specialist
Education Undergraduate: Rutgers College, New Brunswick, NJ
Medical: Medical College of Pennsylvania, Philadelphia, PA Training Orthopaedic Surgery
Residency: Thomas Jefferson University Hospital, Philadelphia, PA Spine
Fellowship: Mayo Clinic, Rochester, MN
Hospital Affiliations Baylor Irving Medical Center Irving Coppell Surgical Center Irving
Offices:
Coppell :
2021 N. MacArthur Blvd 400 West IH 635 Bldg. @, Suite 115
Irving:
Plaza 1, Suite 200
Irving, TX 75061
Irving, TX 75063
Plano:
2301 Marsh Lane,
Plano, TX 75093
Certificates/Diploma’s:











Listing Details

Fax #: (888)238-9155 | E-mail Us

