Posts Tagged ‘science’
You May Get relief from chronic pain by walking
If you are suffering from chronic pain from fibromyalgia or another medical condition, you know the frustration that comes with the attempts to control pain. While medication and therapies are a key factor in pain management, exercise can also work to relieve pain and improve quality of life. Inactivity can lead to more pain – the more you move, the less you will feel your pain.
If you are suffering from chronic pain, begin introducing regular walking workouts into your daily routine. Walking is the most basic form of aerobic exercise. There are several benefits of aerobic exercise, including: building stamina, boosting energy and reducing stiffness and pain. Specific health benefits of walking for exercise include:
- Strengthening muscles – By strengthening the muscles in the feet, legs, hips and torso, you will increase stability of the spine. Spinal stability may reduce symptoms of chronic back pain.
- Improves flexibility and range of motion – With improved range of motion, you will be less susceptible to injury due to stiffness or awkward movements.
- Strengthening joints – A low-impact workout such as walking improves strength and flexibility of the joints, as well as muscles and tendons surrounding the joints.
Research has shown that low-impact aerobic exercise is most effective for improving chronic pain symptoms. It provides a means of relaxation for both the body and mind. Exercise in short intervals has been shown to be most successful in relieving chronic pain. For example, rather than going for one 30-minute walk each day, take three short, 10-minute walks instead.
In a study of 52 sedentary patients with chronic lower back pain, Dr. Michal Katz-Leurer and colleague Ilana Shnayderman found that a simple daily walking routine can improve chronic lower back pain symptoms. Katz-Leurer, from Tel Aviv University’s Stanley Steyer School of Health Professions at the Sackler Faculty of Medicine, and Shnayderman, a graduate student at the Department of Physical Therapy and a practicing physiotherapist at Maccabi Health Care, published their findings in the journal Clinical Rehabilitation.
If you suffer from chronic pain, make a point to exercise daily. By exercising, you will help prevent muscle atrophy and decrease joint pain. Start with a simple 30-minutes of exercise each day, gradually increasing if you are able.
Consult with your physician before beginning any exercise routine.
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us http://www.becomepainfree.com

Share this:

LIVING WITH BACK PAIN
In most instances, individuals with low back pain will improve over a two- to six-week period. The goal is to minimize recurrences and, while being in good physical condition does not prevent all back pain episodes, it will make the resolution of those episodes easier. If you smoke, stop. Smoking is a predisposing factor for back pain. If you are overweight, get into shape. Obesity does not cause back pain, but it does make it harder to heal. (No particular diet is known to prevent episodes of low back pain.) Bottom line, pay attention to your body and exercise, eat right and maintain a healthy life style.
POINTS TO REMEMBER
- Low back pain is a common problem and rarely associated with a severe illness.
- The vast majority of individuals heal back pain by remaining active and taking pain-relieving drugs.
- About 50 percent of individuals are healed in a week or two; over 90 percent are resolved in eight weeks.
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us

Share this:

Stem Cells for Spine Surgery: 7 Points
Written by Laura Miller | May 23, 2012
Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us
How we got here
Dr. Hynes was one of the many spine surgeons who participated in Medtronic’s original trials for BMP-2 in the 1990’s. While scientists have known about the ability of stem cells and BMP to generate bone for several years, Medtronic was the first company to develop a safe and effective molecule to stimulate cell growth. After completing the pre-market approval trials, the Food and Drug Administration granted approval for the BMP-2 product, Infuse, in 2002 for creating fusion in the Lumbar Spine placed through an anterior approach in a LT cage.
“In the original study, I experienced 100 percent of enrolled patients in my Practice achieving bone growth when combining BMP with the local cells that were already there,” says Dr. Hynes. “Local ‘stem cells’ respond to BMP and become activated thereby creating bone. When I saw it worked in 100 percent of my enrolled patients, I was a true believer. I have used it in my practice since the study and FDA approval going back greater than 10 years.”
What has changed is our ability to concentrate stem cells; Dr. Hynes harvests the stem cells from the iliac crest to combine with the BMP. It takes less than five minutes for his physician’s assistant to harvest the cells, which are spun in a centrifuge while he begins the operation. After 10-15 minutes, the cells are ready and Dr. Hynes adds a small amount to the surgical field along with the BMP. The collagen sponge is placed within an interbody LT cage to keep the material from migrating.
“This has been an effective Bone Graft method and it has been an advantage for my patients who can avoid Iliac Bone Graft surgery and Donor Bone issues and cost,” says Dr. Hynes. “It doesn’t add to my usual procedure time. It does add a small cost, but I find it’s worth the value proposition.”
Since its inception and release, surgeons have been experimenting with its use in several different capacities, on- and off-label. However, articles published in The Spine Journal in July 2011 suggest complication rates may be higher than the original studies reported. Several physicians have reported positive and negative events based on individual practice date, and further research into its use will be necessary going forward. As with all products, on label and off label use is routine practice and common place. When used correctly, minimal side effects of swelling, seroma and osteolysis occur.
What the research says
There have been several clinical studies and basic science research projects published in professional journals discussing the efficacy of using BMP with local stem cells to enhance fusion. However, research on the impact of increasing the number of stem cells is still lacking. Dr. Hynes’ current clinical work focuses on whether there is a better chance of achieving fusion with a higher concentration of stem cells.
He harvests stem cells from the iliac crest, percutaneously and painlessly, or vertebral body and extract about 60-80 ccs of blood. The desired stem cells are concentrated to a few ccs with centrifugation and has about a 50,000 cell count per “Spine Smith research data.”
“We already know the mechanism by which BMP-2 activates stem cells. The stem cells are already very effective,” says Dr. Hynes. “If we add to the population of stem cells that are already there that are available to regenerate new bone, it could make the procedure even better. Anecdotally, I have a high fusion rate for my spine patient population even before adding the extra concentration of stem cells. With the additional stem cells, I hope to achieve fusion at almost any level no matter how many levels are needed such as in degenerative scoliosis. In osteoporosis and aging spine patients, this has been extremely beneficial when compared to poor iliac crest from bone harvest.
Dr. Hynes’ ethereal practice goal is to someday be able to “guarantee” that they will achieve fusion for every patient who undergoes surgery. This means stabilization. However, fusion does not guarantee “success” of the surgery but increases odds of the surgical success. At this point, he is close, with approximately a 95 percent fusion rate. “What I want to do before I retire is to be able to guarantee a fusion,” he says. “I can’t guarantee pain relief or other clinical outcomes, but I want to be able to confidently guarantee the fusion or stabilization component.”
Options for harvesting stem cells
There are several bone graft options spine surgeons can choose from to achieve a fusion, and in the wake of recent controversies some surgeons are looking for an alternative to using BMP. Surgeons can go back to the traditional fusion method – the iliac crest – or using an allograft. Dr. Hynes says harvesting bone from the iliac crest can leave 30 percent of patients in more pain and add significant surgical time in the OR with increased blood loss. Allografts also have downsides, including graft consistency, quality, processing issues and less potential to achieve fusion than iliac crest or autogenous grafting methods.
“The bone for allografts may not be prepared correctly,” says Dr. Hynes. “We don’t always know the quality or consistency of the allograft compared to the patient’s natural bone. If I’m putting a piece of bone in patients, it’s better if it comes from their own bodies. That way, you can’t tell the difference between the bone you grow and the natural bone. (What we are doing is creating a nice bone graft that balances the biomechanics of the fusion construct better than the allograft.)”
In some cases, the allograft bone could migrate or fracture or reabsorb after the procedure, which can cause significant pain and complications, often resulting in revision procedures. By using the combination of BMP and stem cells in an interbody device, Dr. Hynes is able to avoid most of those complications because the cells are attracted to the BMP, which is restrained in the cage.
Patients should have the final say – “Informed Consent”!
Like many surgeons, Dr. Hynes describes the different fusion options to his patients and allows them to choose which procedure they feel most comfortable with. He discusses the pros and cons of each technique, including the most recent concerns about BMP, as well as his personal outcomes. He says patients often choose BMP combined with stem cells because they like the idea of regenerating their own bone naturally, avoiding the extra surgery and potential pain of iliac crest bone grafts and decreased potential or effect of donor allograft bone.
“The psychology of healing is part of this,” says Dr. Hynes. “Patients understand the procedure and like the idea of using their own cells as healing factors. People are very positive about that process because they feel like they are doing something natural instead of synthetic. Healing and surgery isn’t just biomechanics and science; it’s psychological as well. Successful outcomes of surgery depend on subjective relief as well as objective factors.”
In his practice, Dr. Hynes says a significant number of his patients chose the BMP and stem cell combination with given the option. However, when the patients choose a different option, he performs the other procedures as well. “It’s our duty to give patients their choice,” he says. “I’m not always smart enough to know what the best choice is for any one individual, but I’ve practiced many years and learned that if you take time to educate patients to all the reasonable options, they will make good decisions and take responsibility for them.”
Deciphering the complications
While Dr. Hynes hasn’t experienced significant complications among his patients, it’s clear that other surgeons have reported complications when they perform spinal fusions using BMPs. One reason for the discrepancy could be the dosage; well-documented evidence suggests that a higher dosage of BMP could cause swelling complications when used in the cervical spine. By using low doses of BMP and a pre and post-surgical protocol, swelling is completely avoidable in the cervical spine. Another factor is the surgical approach; Dr. Hynes says retrograde ejaculation (“RE”) – one of the severe complications mentioned in the studies this past summer – is a complication risk of any anterior spine surgery and not related to use of BMP. “I have performed thousands of anterior procedures before and after approval of BMP for anterior lumbar surgery and I find no difference in RE noted in my patients.”
“Every spine surgeon knows RE is a risk during anterior procedures and it usually will reverse on its own,” says Dr. Hynes. “RE occurs in an extremely low frequency. RE occurs because of disruption ‘surgically’ of small nerves to a sphincterine the bladder. BMP does not cause this effect, but the use of the electrocautery tool, during surgery, likely does. Use a small dose of BMP and a cage as well.”
In his practice, Dr. Hynes has never experienced a critical airway complication using cervical BMP. In early years, too high a dose would lead to swelling but not airway compromise which more commonly occurs with hematoma or blood clot, says Dr. Hynes. Papers published in The Spine Journal also mention cancer as an associated complication, which is something he hasn’t necessarily noted either. “I haven’t seen a rash of cancer in my patients, but I haven’t been surveying for it either,” he says.
He is currently going through his patient base to determine whether he can detect any cancer cases that could be associated with the procedure.
Whether to use BMPs
As surgeons report different findings based on their individual practice data, many of the studies and discrepancies have been reported in the media. However, full understanding of these complex issues is often lost in news reports. “I hate to see some of the surgeons and journals duking it out in the media,” says Dr. Hynes. “That isn’t the place to argue over the efficacy of stem cells and BMPs. We have to do it in the meetings where people understand the context. To lay this out in the newspapers exacerbates political agendas and confuses our patients. We need to speak honestly with each other about this at professional and scientific meetings, not in the press.”
This controversy isn’t the first time new spinal technology and procedures have been under attack. For a period of time, pedicle screws – which are a standard of care now – were under the microscope because complications were reported. In some instances, surgeons were sued and restricted from use at their hospitals for their alleged unfavorable outcomes. Now pedicle screws are the mainstay of spinal fusion procedures.
“At the time, there was only approval that pedicle screws could be used on single-level surgeries,” says Dr. Hynes. “Now we use them at multi-levels. The pedicle screws ultimately won the day, but with public stimulation ‘in the news’ in the early 1990s, we almost lost the ability to use them. This was a public attack on the advent of a new fusion technology, and now we are seeing similar phenomenon’s with BMP and other medical products.”
Covering the cost of BMP
In some cases, surgeons may have a difficult time receiving reimbursement for BMP products because they were more expensive in the past. Dr. Hynes and his colleagues have worked with hospitals and surgery centers to cover the cost in both out-of-network and in-network contracts. In some cases, patients are willing to cover the cost of using stem cells with BMP. Due to the success and demand, the cost has now become competitive considering operative costs of iliac bone surgery or allograft. “The increased volume of use and effectiveness has caused a dramatic decrease in cost,” says Dr. Hynes.
“I see patients from out of the Country and they are usually cash pay patients,” says Dr. Hynes. “We have to line item every part of the procedure to show the actual cost and there is almost no increased cost for the use of low concentrated BMP compared to iliac bone grafts or allograft when taking OR time, surgeon’s time and other OR costs into consideration.”
Fortunately, the hospitals in Dr. Hynes’ community allowed him to use BMP and conduct the clinical studies there. “We have more experience in our community with the benefits of this technology because we started so early,” he says. “Our surgeries are very efficient and our operative time is less because of our long-term experience with the procedure using stem cells and BMP.”
However, in some cases Dr. Hynes has made sacrifices to mitigate these costs. “I think about what I could live without and forego those expenses for stem cells and BMP,” he says. “I might use less expensive blades or a new set of tools for the next year. I might continue to use my old led apron or do surgery without a super drape. I’m there to give patients a better outcome and I want to make sure they have the opportunity to have the stem cells.”
More Articles on Spine Surgeons:
8 Spine Surgeons on the Future of Spinal Fusions
6 Spine Surgeons on How Young Surgeons Can Position Themselves for Success in the Future
What Percentage of Your Spine Practice is Medicare Patients?
Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us
Share this:

Top Orthopedic Surgeons in Texas, Top Back Surgeons in Texas, Top Spine Surgeons in Texas
Looking for an Orthopedic surgeon that you can trust is a daunting task. You do not want to chance that the person you are going to for ankle, knee, hip, or even spinal surgery may not be among the best in their field. Though this is a decision you have to make for yourself after meeting the orthopedic surgeons in person we are giving you a good start. Hopefully an end to your frustration even.
Orthopedic surgery is becoming ever more common as advancements allow for better hip and knee replacements which of course makes the demand for orthopedic surgeons higher. Find the best ones in Texas so you can find the surgeon that is right for you and your needs. Something as important as a hip replacement or any other orthopedic surgery, can’t be left to chance and all the time spent researching surgeons around can take up an awful lot of time. So here are the top orthopedic surgeons we have chosen in Texas.
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us

Steven J. Cyr, M.D.
San Antonio, TXDr. Steven Cyr, is a Board Certified Orthopaedic Surgeon who received extensive training to specialize in the delicate science of Spine Surgery. He has brought innovative techniques to the military and was the first to perform the total disc replacement procedure as well as endoscopic spinal surgery. He specializes in complicated spine issues and has gained notoriety for successful repairs of failed surgeries on patients from numerous other states and around the world.

2504 Ridge Road, #206, Rockwall, Texas, United States, 75087
Dr. Mike-Mayer is a fellowship trained Orthopaedic Spine Surgeon specializing in the non-operative and surgical treatment of spinal disorders. He completed his undergraduate degree at Drake University. He earned …
 Dallas,, Tx, United States
Dallas,, Tx, United States
Neil Dilip Shah, MD is a Board-Eligible Orthopedic Surgeon and Fellowship-Trained Spine Surgery. Dr. Shah brings a conservative approach to low back and neck pain while also offering the most current minimally invasive surgical techniques when a procedure …
 2021 N. MacArthur Blvd, Irving, Tx, 75061
2021 N. MacArthur Blvd, Irving, Tx, 75061
Mayo Fellowship Trained Board-Certified Spine Surgeon Minimally Invasive Spine Specialist Education Undergraduate: Rutgers College, New Brunswick, NJ Medical: Medical College of Pennsylvania, Philadelphia, PA Training Orthopaedic Surgery Residen …
 14450 T C Jester Boulevard #100, Houston, TX, 77014
14450 T C Jester Boulevard #100, Houston, TX, 77014
BOARD ELIGIBLE ORTHOPEDIC and SPINE SURGEON Dr Siddiqui is proficient in treating cervical, thoracic and lumbar spinal conditions and disorders whether they require surgical treatment or non-operative treatment. Degenerative disc disease is a common pro …
 2900 N I-35, Ste 110, Denton, Tx, USA, 76201
2900 N I-35, Ste 110, Denton, Tx, USA, 76201
Dr. Eric Gioia has been practicing neurosurgeon in Texas for over 20 years. A graduate of the University of Mississippi Medical School (1979), Dr. Gioia completed his neurosurgical residency at the University of Tennessee, Memphis (1985) and served his su …
 3900 Junius St., Dallas, Texas, 75246
3900 Junius St., Dallas, Texas, 75246
Dr. Huntly Chapman is an fellowship trained Orthopedic Spine surgeon, specializing in the treatment of low back and neck pain. Dr. Chapman utilizes both conservative non-operative and surgical treatments. Dr. Chapman received his medical degree from th …
 3625 Camp Bowie Boulevard, Fort Worth, TX, USA, 76107
3625 Camp Bowie Boulevard, Fort Worth, TX, USA, 76107
Dr. Kaufman is a specialist in cerebrovascular, skull base and complex spine surgery. He has published numerous articles, manuscripts and abstracts on subjects such as brain tumors and complex spinal surgery. He has also made presentations on skull base a …
 431 Omega Dr. #104, Arlington, TX, USA, 76014
431 Omega Dr. #104, Arlington, TX, USA, 76014
Dr. John Sazy is a fellowship trained Orthopaedic Surgeon with extensive training in Spine Surgery with offices in Arlington and Fort Worth, Texas. Dr. Sazy evaluates for and performs reconstructive spine surgery, revision spine surgery, scoliosis surger …
 16929 Southwest Freeway, Suite 100, Sugarland, TX, 77479
16929 Southwest Freeway, Suite 100, Sugarland, TX, 77479
Orthopaedic Spine Surgeon Board Certified/Fellowship Trained Surgery of the Cervical, Thoracic, and Lumbar Spine Kenneth J.H. Lee, M.D. Born in Chicago, Illinois and a native of North Carolina, Dr. Kenneth Lee graduated from Duke Universi …
 2301 S Hampton Rd Suite 800, Dallas, TX, USA, 75224
2301 S Hampton Rd Suite 800, Dallas, TX, USA, 75224
Orthopedic spine surgery
 399 W. Campbell Rd. #408, Richardson, TX, USA, 75080
399 W. Campbell Rd. #408, Richardson, TX, USA, 75080
Knee/Lumbar Spine Surgery
 3600 W 7th St, Fort Worth, TX, USA, 76107
3600 W 7th St, Fort Worth, TX, USA, 76107
Dr. Henry earned his Doctorate of Osteopathic Medicine from Ohio University. He participated in a traditional rotating internship and an Orthopedic Surgery through Ohio University. Dr. Henry’s fellowship work was completed with the Texas Back Institut …
 5228 W. Plano Pkwy, Plano, TX, United States, 75093
5228 W. Plano Pkwy, Plano, TX, United States, 75093
As a highly skilled specialist in surgical procedures involving the spine, Dr. Stephen P. Courtney has established an excellent reputation with his professional colleagues and patients. He is a board-certified, fellowship- trained orthopedic spine sur …
 7777 Forest Lane, Bldg. C, Suite 500, Dallas, TX, 75230
7777 Forest Lane, Bldg. C, Suite 500, Dallas, TX, 75230
Dr. Zach Kelley is a fellowship trained spine surgeon who specializes in minimally invasive spine procedures. Patients who have minimally invasive spine procedures have smaller incisions, less blood loss, and a shorter hospital stay. Dr. Zach Kelley co …
Share this:

Regenerative Medicine
Administering undifferentiated stem cells to an injured disc has made adult stem cell regenerative medicine in spine a reality. Adult stem cell regenerative medicine holds the promise of stabilizing or even reversing the degenerative changes associated with aging or following traumatic injury. Current clinical use of stem cells is very limited, in part by the cumbersome approval process. The use of concentrated bone marrow aspirate (BMC) as a “stem cell” preparation is currently the simplest and safest way of utilizing the regenerative potential for mesenchymal stem cells (MSCs) to promote tissue regeneration. In fact, stem cells concentrated from bone marrow have been shown to stimulate the formation of bone, cartilage, ligament and tendon, and dermal tissues.
Conservative treatment options for lumbar and cervical pain associated with discogenic disc disease (Pfirrmann Grades 3-6) are limited. Treatment options include pain medication, steroids, physical therapy, and chiropractic care. Reversal of disc pathology has not been achieved with current available treatment modalities. Failure of these nonoperative treatments may leave surgical intervention as a treatment option.
The goal of utilizing MSCs is to not only potentially provide pain relief from the painful degenerative disc, but to reverse the degenerative process. There are three methods for placing MSCs into the painful nucleus pulposus.
The use of allogeneic mesenchymal precursor cells (MPCs) is currently being evaluated as a part of an FDA Phase I clinical trial. Extracted from donors and expanded in number by tissue culture, this process isolates and grows the stem cells into pure MPCs which are injected into the nucleus pulposus. This technology does not have FDA approval.
Utilizing expanded, autologous MSCs for injection into the painful disc is the second method. Federal regulations require the approval of an Investigational New Drug application supported by prospective, randomized clinical trials for the use of expanded autologous MSCs. The FDA has not approved this technology.
The third method involves autologous point of care therapy. This technology does not require FDA approval. The patient’s own MSCs are directly injected into the nucleus pulposus of the symptomatic degenerated disc(s) using standardized two needle discography technique. This requires fluoroscopic visualization and 2-3cc of MSCs are slowly injected into the symptomatic nucleus pulposus.
There have been no complications associated with the iliac crest aspiration or disc injection. Thus far no patient in the study has undergone spine surgery following treatment. Results obtained with this technique suggest its potential clinical efficacy in the treatment of moderate to severe degenerative disc disease. These results require verification with longer follow-up and randomized prospective studies.
For more information regarding treatment options please visit our websites at http://www.becomepainfree.com
Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us
Share this:

Adult Stem Cell Therapy to Treat Back Pain, Stem Cell, Spine Stem Cells, Stem Cell Treatment
Adult Stem Cell Therapy that doesn’t require FDA approval to treat lumbar and cervical spine conditions resulting from injury or aging, and is also involved with an FDA clinical trial investigating the use of Adult Stem Cells.
Stem Cell
These stem cells are autologous – they are taken from an adult patient and returned to that same patient in a concentrated form to the damaged area in a 30-minute procedure. This type of adult stem cell therapy does not require FDA approval to administer.
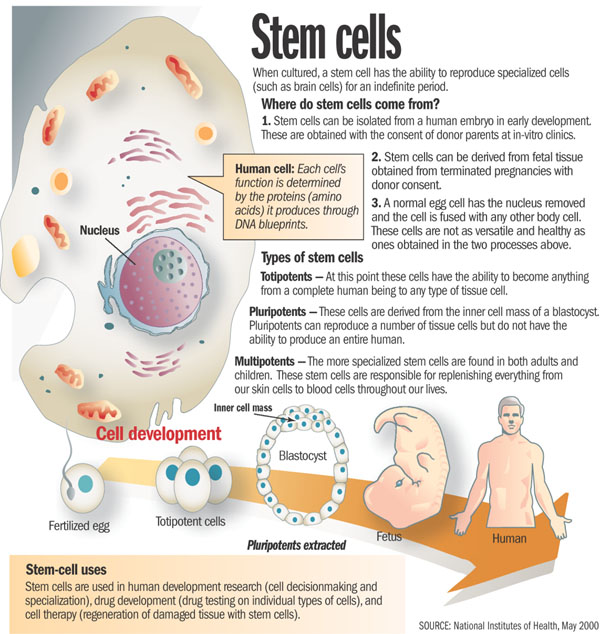
When it comes to stem cells, there is often a lot of mystique surrounding them. We hear from the media that we can create a human being out of a bundle of cells, which is not necessarily true. We also tend to look at embryonic stem cells as being the only type of stem cell. With these types of embryonic stem cells, one idea is to be able to create a liver or kidney in a Petri dish, which is not controllable or feasible at this point, and the work being done by the BecomePainFree.com medical group.
When we look at stem cell types, we have embryonic stem cells on one hand and adult stem cells on the other. The characteristics of each of these are not like other cells. For instance, a liver cell can divide but it will only ever be a liver cell. These stem cells, both embryonic and adult, can turn into different types of cells. The embryonic stem cells can really turn into any cell type, but adult stem cells are limited as far as the cells they can turn into. This depends upon environment or niche and what they are already programmed to become. A lot of people think there is a lot of promise with embryonic stem cells and there is, although we are not quite there yet.
We are still at the forefront of stem cell technology and embryonic stem cells in particular. With those cells, we do not have the ability to control what types of tissue they turn into. For example, we could be trying to manipulate these cells to turn into kidneys, but they might start to develop as pancreatic cells, which is troublesome. Another key with all stem cells is that they can proliferate quite a bit, usually at a higher rate than just a regular somatic cell. Although this sounds good at first glance, the issue with this, particularly with embryonic stem cells, is we cannot control that division. Hence, these cells can keep going and going without dying. In the normal bodily process, cells are programmed to die after a certain time, but these embryonic stem cells can evade that action and continue dividing, which takes on the characteristic of cancer cells. In some animal studies, an issue that keeps arising is development of tumors in some of these animals. It is difficult to predict if tumors are going to form when using some sort of embryonic stem cell treatment. This is still a scary area through which we are still trying to navigate.
However, the focus of the BecomePainFree.com medical group is on adult mesenchymal stem cells. On the whole, the media does not give a lot of attention to these kinds of stem cells, as using them avoids any kind of ethical or controversial issues. There is a great amount of research being done on adult mesenchymal stem cells, however, because they are very powerful.
First off, we can control what cell type they turn into much more easily. For example, the treatment used by the BecomePainFree.com medical group focuses on Mesenchymal precursor cells (MPC). Mesenchymal means these cells are not going to turn into any kind of blood product such as a red blood cell or white blood cell, although they are derived from bone marrow. The fact that they are precursor cells means these MPCs are only going to differentiate into one of a few cell types. They are either going to become bone cells, i.e., osteoblasts, or chondrocytes, i.e., cartilaginous tissue such that we see in intervertebral discs and joints, etc. All of that really depends on the environment in which we place these adult stem cells where it is well suited to do this. For example, we can inject these MPCs into a bone fracture, and because the cells are surrounded by bone tissue, these cells will receive signals from the surrounding cells that tell them to turn into bone. However, the cells we use will be injected into a disc or joint, and the cells composing the disc and joint tissue will signal the stem cells to develop into similar tissue. Again, there is no chance of any sort of pancreatic cell or nerve cell type spontaneously forming because we are using certain adult stem cell types, which are limited and cannot turn into anything like that. In addition, as the tissue surrounding the disc and joint is relatively avascular, there is not really any worry of these cells migrating through the blood stream to somewhere else in the body and causing any sort of problem. As far as the proliferation issue with embryonic stem cells, we have not seen this issue with adult stem cells in terms of dividing exponentially without ceasing. There is almost a preset limit to how many times these adult stem cells will divide.
Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us https://www.becomepainfree.com/
Share this:

Dr. Henrik Mike-Mayer, M.D., Texas Back Institute, Texas Back Institute Fellow, TBI, Rockwall Spine Surgeon, Rockwall Pain Doctor
Dr. Henrik Mike-Mayer, M.D.
https://www.becomepainfree.com/
Dr. Mike-Mayer is a fellowship trained Orthopaedic Spine Surgeon specializing in the non-operative and surgical treatment of spinal disorders. He completed his undergraduate degree at Drake University. He earned his medical degree at the University of Medicine and Dentistry – New Jersey Medical School. He received his Orthopaedic training and was Chief Resident at the Seton Hall University School of Graduate Medical Education in New Jersey. He completed a one year spine fellowship in Disorders of the Spine at Texas Back Institute. During this fellowship, he was exposed to the most complex spinal disorders and received training in the newest cutting-edge techniques and equipment. He continues to pursue training in the latest developments in spine surgery and is involved in clinical research including FDA IDE trials.
At BecomePainFree.com doctors group, our commitment to our patients is the highest level of personal and comprehensive attention and care.
To ensure the highest quality of patient care, Dr. Mike-Mayer and his staff carefully and thoroughly evaluate each and every patient’s condition and provide the highest level of non-operative and surgical care necessary to improve spinal health. Dr. Mike-Mayer manages a wide-range of spinal cases from children, adult and geriatric patients, injured workers and sports injuries.

Listing Details

Become Pain Free | Pain Specialist in Texas
Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us https://www.becomepainfree.com/
Share this:

Minimally Invasive Stabilization (MIS), Cervical Spine Anterior Cervical Discectomy and Stabilization (ACDS)
Anterior Cervical Discectomy and Stabilization (ACDS) is a type of minimally invasive fusion surgery that may be helpful in treating the following conditions within the cervical (neck) spine presented by BecomePainFree:

About ACDS
The ACDS procedure is designed to relieve neck pain by removing your painful disc material and bone spurs. During the ACDS procedure, the damaged disc is removed and implants are inserted to help stabilize your bones.
Like the other types of minimally invasive surgery at BecomePainFree.com, ACDS is performed through a small incision with the use of a surgical telescope. This approach eliminates the need to cut through muscle and involves minimal soft tissue damage, resulting in a quicker recovery for most patients.
Through a small incision, the surgeon will make a tunnel to the spine through the front area of the neck by moving aside muscles so that the bony vertebrae and discs can be seen. With the aid of a fluoroscope (a special X-ray), the surgeon will remove the disc and the remaining disc material. Next, open disc space is prepared for the bone graft stabilization or the artificial disc replacement. Allograft bone, or bone taken from your hip area, is used to complete the reconstruction and is then stabilized with a small titanium plate. Once that is complete, the incision is closed and the patient is on their way to postoperative recovery.
Call our group today Call Us: (214) 396-3647 | (888) 373-3720 Fax #: (888 )238-9155 | E-mail Us
https://www.becomepainfree.com/
Share this:

Anterior cervical discectomy & fusion (ACDF), ACDF, ACDF Spine Surgery
 ACDF Spine/Back Surgery Overview
ACDF Spine/Back Surgery Overview

Come see on of our Doctors today please visit https://www.becomepainfree.com/
Anterior cervical discectomy and fusion (ACDF) is a surgical procedure performed to remove a herniated or degenerative disc (Fig. 1) in the cervical (neck) spine. The surgeon approaches the spine from the front, through the throat area. After the disc is removed, the vertebrae above and below the disc space are fused together. Your doctor may recommend a discectomy if physical therapy or medication fail to relieve your neck or arm pain caused by inflamed and compressed spinal nerves. Patients typically go home the same day; recovery time takes 4 to 6 weeks.
Spine Surgery
Figure 1, top. (top view of vertebra) Degenerative disc disease causes the discs (purple) to dry out. Tears in the disc annulus can allow the gel-filled nucleus material to escape and compress the spinal cord causing numbness and weakness. Bone spurs may develop which can lead to a narrowing of the nerve root canal (foraminal stenosis). The pinched spinal nerve becomes swollen and painful.
What is an anterior cervical discectomy & fusion (ACDF)?
Discectomy literally means “cutting out the disc.” A discectomy can be performed anywhere along the spine from the neck (cervical) to the low back (lumbar). The surgeon reaches the damaged disc from the front (anterior) of the spine — through the throat area. By moving aside the neck muscles, trachea, and esophagus, the disc and bony vertebrae are accessed. In the neck area of the spine, an anterior approach is more convenient than a posterior (back) because the disc can be reached without disturbing the spinal cord, spinal nerves, and the strong neck muscles of the back. Depending on your particular case, one disc (single-level) or more (multi-level) may be removed.
After the disc is removed, the space between the bony vertebrae is empty. To prevent the vertebrae from collapsing and rubbing together, the surgeon fills the open disc space with a bone graft. The graft serves as a bridge between the two vertebrae to create a spinal fusion. The bone graft and vertebrae are often immobilized and held together with metal plates and screws. Following surgery the body begins its natural healing process and new bone cells are formed around the graft. After 3 to 6 months, the bone graft should join the vertebrae above and below to form one solid piece of bone. With instrumentation and fusion working together, the bone may actually grow around the plates and screws – similar to reinforced concrete.
Bone grafts come from many sources. Each type has advantages and disadvantages.
- Autograft bone comes from you. The surgeon takes your own bone cells from the hip (iliac crest). This graft has a higher rate of fusion because it has bone-growing cells and proteins. The disadvantage is the pain in your hipbone after surgery. Harvesting a bone graft from your hip is done at the same time as the spine surgery. The harvested bone is about a half inch thick – the entire thickness of bone is not removed, just the top half layer.
- Allograft bone comes from a donor (cadaver). Bone-bank bone is collected from people who have agreed to donate their organs after they die. This graft does not have bone-growing cells or proteins, yet it is readily available and eliminates the need to harvest bone from your hip. Allograft is shaped like a doughnut and the center is packed with shavings of living bone tissue taken from your spine during surgery.
- Bone graft substitute comes from man-made plastic, ceramic, or bioresorbable compounds. Often called cages, this graft material is packed with shavings of living bone tissue taken from your spine during surgery.
After fusion you may notice some range of motion loss, but this varies according to neck mobility before surgery and the number of levels fused. If only one level is fused, you may have similar or even better range of motion than before surgery. If more than two levels are fused, you may notice limits in turning your head and looking up and down. New motion-preserving artificial disc replacements have emerged as an alternative to fusion. Similar to knee replacement, the artificial disc is inserted into the damaged joint space and preserves motion, whereas fusion eliminates motion. Outcomes for artificial disc compared to ACDF (the gold standard) are similar, but long-term results of motion preservation and adjacent level disease are not yet proven. Talk with your surgeon about whether ACDF or artificial disc replacement is most appropriate for your specific case.
Who is a candidate?
You may be a candidate for discectomy if you have:
- diagnostic tests (MRI, CT, myelogram) show that you have a herniated or degenerative disc
- significant weakness in your hand or arm
- arm pain worse than neck pain
- symptoms that have not improved with physical therapy or medication
ACDF may be helpful in treating the following conditions:
- Bulging and herniated disc: The gel-like material within the disc can bulge or rupture through a weak area in the surrounding wall (annulus). Irritation and swelling occurs when this material squeezes out and painfully presses on a nerve.
- Degenerative disc disease: As discs naturally wear out, bone spurs form and the facet joints inflame. The discs dry out and shrink, losing their flexibility and cushioning properties. The disc spaces get smaller. These changes lead to foraminal or central stenosis or disc herniation (Fig. 1).

The surgical decision
Most herniated discs heal after a few months of nonsurgical treatment. Your doctor may recommend treatment options, but only you can decide whether surgery is right for you. Be sure to consider all the risks and benefits before making your decision. Only 10% of people with herniated disc problems have enough pain after 6 weeks of nonsurgical treatment to consider surgery.
Your surgeon will also discuss the risks and benefits of different types of bone graft material. Autograft is the gold standard for rapid healing and fusion, but the graft harvest can be painful and at times lead to complications. Autograft is more commonly used these days as it has proven to be as effective for routine 1 and 2 level fusions in non-smokers.
Who performs the procedure?
A neurosurgeon or an orthopedic surgeon can perform spine surgery. Many spine surgeons have specialized training in complex spine surgery. Ask your surgeon about their training, especially if your case is complex or you’ve had more than one spinal surgery.
What happens before surgery?
You may be scheduled for presurgical tests (e.g., blood test, electrocardiogram, chest X-ray) several days before surgery. In the doctor’s office, you will sign consent and other forms so that the surgeon knows your medical history (allergies, medicines/vitamins, bleeding history, anesthesia reactions, previous surgeries). Discuss all medications (prescription, over-the-counter, and herbal supplements) you are taking with your health care provider. Some medications need to be continued or stopped the day of surgery.
Stop taking all non-steroidal anti-inflammatory medicines (Naprosyn, Advil, Motrin, Nuprin, Aleve, etc.) and blood thinners (Coumadin, Plavix, etc.) 1 to 2 weeks before surgery as directed by the doctor. Additionally, stop smoking, chewing tobacco, and drinking alcohol 1 week before and 2 weeks after surgery because these activities can cause bleeding problems. No food or drink is permitted past midnight the night before surgery.
Smoking
The most important thing you can do to ensure the success of your spinal surgery is quit smoking. This includes cigarettes, cigars, pipes, chewing tobacco, and smokeless tobacco (snuff, dip). Nicotine prevents bone growth and puts you at higher risk for a failed fusion. Patients who smoked had failed fusions in up to 40% of cases, compared to only 8% among non-smokers [1]. Smoking also decreases your blood circulation, resulting in slower wound healing and an increased risk of infection. Talk with your doctor about ways to help you quit smoking: nicotine replacements, pills without nicotine (Wellbutrin, Chantix), and tobacco counseling programs.
Morning of surgery
- Shower using antibacterial soap. Dress in freshly washed, loose-fitting clothing.
- Wear flat-heeled shoes with closed backs.
- If you have instructions to take regular medication the morning of surgery, do so with small sips of water.
- Remove make-up, hairpins, contacts, body piercings, nail polish, etc.
- Leave all valuables and jewelry at home (including wedding bands).
- Bring a list of medications (prescriptions, over-the-counter, and herbal supplements) with dosages and the times of day usually taken.
- Bring a list of allergies to medication or foods.
Arrive at the hospital 2 hours before (surgery center 1 hour before) your scheduled surgery time to complete the necessary paperwork and pre-procedure work-ups. An anesthesiologist will talk with you and explain the effects of anesthesia and its risks. An intravenous (IV) line will be placed in your arm.
What happens during surgery?
There are seven steps to the procedure. The operation generally takes 1 to 3 hours.
Step 1: prepare the patient
You will lie on your back on the operative table and be given anesthesia. Once asleep, your neck area is cleansed and prepped. If a fusion is planned and your own bone will be used, the hip area is also prepped to obtain a bone graft. If a donor bone will be used, the hip incision is unnecessary.
Step 2: make an incision
A 2-inch skin incision is made on the right or left side of your neck (Fig. 2). The surgeon makes a tunnel to the spine by moving aside muscles in your neck and retracting the trachea, esophagus, and arteries. Finally, the muscles that support the front of the spine are lifted and held aside so the surgeon can clearly see the bony vertebrae and discs.

Figure 2. A 2-inch skin incision is made on the side of your neck.
Step 3: prepare to remove disc
With the aid of a fluoroscope (a special X-ray), the surgeon passes a thin needle into the disc to locate the affected vertebra and disc.
To remove the damaged disc, the vertebrae above and below the disc must be held apart. Your surgeon first inserts a spreader into the body of each vertebra above and below the disc to be removed. Gentle tension is placed on the spreader to separate the two vertebrae.
Step 4: remove the disc fragments
The outer wall of the disc (annulus) is cut (Fig. 3). The surgeon removes about 2/3 of your disc using small grasping tools, and then looks through a surgical microscope to remove the rest of the disc. The posterior longitudinal ligament, which runs behind the vertebrae, is removed to reach the spinal canal. Any disc material pressing on the spinal nerves is removed.
Figure 3. The muscles are retracted to expose the vertebra. The disc annulus is cut open and the disc material is removed with grasping tools.
Step 5: decompress the nerve
Bone spurs (osteophytes) that press on your nerve root are removed. The foramen, through which the spinal nerve exits, is enlarged with a drill (Fig. 4). This procedure, called a foraminotomy, gives your nerves more room to exit the spinal canal.

Figure 4. (top view) The disc annulus and nucleus are removed to decompress the spinal cord and nerve root. Bone spurs are removed and the spinal foramen is enlarged to free the nerve.
Step 6. prepare a bone graft fusion
Using a drill, the open disc space is prepared on the top and bottom by removing the outer cortical layer of bone to expose the blood-rich cancellous bone inside. This “bed” will hold the bone graft material that you and your surgeon selected:
- Bone graft from your hip. A skin and muscle incision is made over the crest of your hipbone. Next, a chisel is used to cut through the hard outer layer (cortical bone) to the inner layer (cancellous bone). The inner layer contains the bone-growing cells and proteins. The bone graft is then shaped and placed into the “bed” between the vertebrae (Fig. 5).
- Bone bank or fusion cage. A cadaver bone graft or bioplastic cage is filled with the leftover bone shavings containing bone-growing cells and proteins. The graft is then tapped into the shelf space.

Figure 5. (side view) A bone graft (blue) is shaped and inserted into the shelf space between the vertebrae.
The surgeon may reinforce the bone graft with a metal plate screwed into the vertebrae to provide stability during fusion – and possibly a better fusion rate. An x-ray is taken to verify the position of the bone graft and the metal plate and screws (Fig. 6).
Come see on of our Doctors today please visit https://www.becomepainfree.com/
New option: artificial disc replacement. Instead of a bone graft or fusion cage, an artificial disc device is inserted into the empty disc space. In select patients, it may be beneficial to preserve motion. Talk to your doctor – not all insurance companies will pay for this new technology and out-of-pocket expenses may be incurred.
Step 7. close the incision
The spreader and retractors are removed. The muscle and skin incisions are sewn together with sutures. Steri-Strips or biologic glue is placed across the incision.
What happens after surgery?
You will awaken in the postoperative recovery area, called the PACU. Blood pressure, heart rate, and respiration will be monitored. Any pain will be addressed. Once awake, you will be moved to a regular room where you’ll increase your activity level (sitting in a chair, walking). Patients who have had bone graft taken from their hip may feel more discomfort in their hip than neck incision. Most patients having a 1 or 2 level ACDF are sent home the same day. However, if medical complications such as difficulty breathing or unstable blood pressure develop, you may need to stay overnight. You will be given written instructions to follow when you go home.
Discharge instructions

Discomfort
- After surgery, pain is managed with narcotic medication. Because narcotic pain pills are addictive, they are used for a limited period (2 to 4 weeks). As their regular use can cause constipation, drink lots of water and eat high fiber foods. Laxatives (e.g., Dulcolax, Senokot, Milk of Magnesia) can be bought without a prescription. Thereafter, pain is managed with acetaminophen (e.g., Tylenol).
- Hoarseness, sore throat, or difficulty swallowing may occur in some patients and should not be cause for alarm. These symptoms usually resolve in 1 to 4 weeks.
Restrictions
- If you had a fusion, do not use non-steroidal anti-inflammatory drugs (NSAIDs) (e.g., aspirin; ibuprofen, Advil, Motrin, Nuprin; naproxen sodium, Aleve) for 6 months after surgery. NSAIDs may cause bleeding and interfere with bone healing.
- Do not smoke. Smoking delays healing by increasing the risk of complications (e.g., infection) and inhibits the bones’ ability to fuse.
- Do not drive for 2 to 4 weeks after surgery or until discussed with your surgeon.
- Avoid sitting for long periods of time.
- Avoid bending your head forward or backward.
- Do not lift anything heavier than 5 pounds (e.g., gallon of milk).
- Housework and yard-work are not permitted until the first follow-up office visit. This includes gardening, mowing, vacuuming, ironing, and loading/unloading the dishwasher, washer, or dryer.
- Postpone sexual activity until your follow-up appointment unless your surgeon specifies otherwise.
Activity
- You may need help with daily activities (e.g., dressing, bathing), but most patients are able to care for themselves right away.
- Gradually return to your normal activities. Walking is encouraged; start with a short distance and gradually increase to 1 to 2 miles daily. A physical therapy program may be recommended.
- If applicable, know how to wear a cervical collar before leaving the hospital. Wear it when walking or riding in a car.
Bathing/Incision Care
- You may shower 1 to 4 days after surgery. Follow your surgeon’s specific instructions. No tub baths, hot tubs, or swimming pools until your health care provider says it’s safe to do so.
- If you have staples or stitches when you go home, they will need to be removed. Ask your surgeon or call the office to find out when.
When to Call Your Doctor
- If your temperature exceeds 101° F, or if the incision begins to separate or show signs of infection, such as redness, swelling, pain, or drainage.
- If your swallowing problems interfere with your ability to breathe or drink water.
Recovery and prevention
Schedule a follow-up appointment with your surgeon for 2 weeks after surgery. Recovery time generally lasts 4 to 6 weeks. X-rays may be taken after several weeks to verify that fusion is occurring. The surgeon will decide when to release you back to work at your follow-up visit.
A cervical collar or brace is sometimes worn during recovery to provide support and limit motion while your neck heals or fuses (see Braces & Orthotics). Your doctor may prescribe neck stretches and exercises or physical therapy once your neck has healed.
If you had a bone graft taken from your hip, you may experience pain, soreness, and stiffness at the incision. Get up frequently (every 20 minutes) and move around or walk. Don’t sit or lie down for long periods of time.
Recurrences of neck pain are common. The key to avoiding recurrence is prevention:
What are the results?
Anterior cervical discectomy is successful in relieving arm pain in 92 to 100% of patients [3]. However, arm weakness and numbness may persist for weeks to months. Neck pain is relieved in 73 to 83% of patients [3]. In general, people with arm pain benefit more from ACDF than those with neck pain. Aim to keep a positive attitude and diligently perform your physical therapy exercises.
Achieving a spinal fusion varies depending on the technique used and your general health (smoker). In a study that compared three techniques: ACD, ACDF, and ACDF with plates and screws, the outcomes were [3]:
- 67% of people who underwent ACD (no bone graft) achieved fusion naturally. However, ACD alone results in an abnormal forward curving of the spine (kyphosis) compared with the other techniques.
- 93% of people who underwent ACDF with bone graft placement achieved fusion.
- 100% of people who underwent ACDF with bone graft placement and plates and screws achieved fusion.
What are the risks?
No surgery is without risks. General complications of any surgery include bleeding, infection, blood clots (deep vein thrombosis), and reactions to anesthesia. If spinal fusion is done at the same time as a discectomy, there is a greater risk of complications. Specific complications related to ACDF may include:
Hoarseness and swallowing difficulties. In some cases, temporary hoarseness can occur. The recurrent laryngeal nerve, which innervates the vocal cords, is affected during surgery. It may take several months for this nerve to recover. In rare cases (less than 1/250) hoarseness and swallowing problems may persist and need further treatment with an ear, nose and throat specialist.
Vertebrae failing to fuse. Among many reasons why vertebrae fail to fuse, common ones include smoking, osteoporosis, obesity, and malnutrition. Smoking is by far the greatest factor that can prevent fusion. Nicotine is a toxin that inhibits bone-growing cells. If you continue to smoke after your spinal surgery, you could undermine the fusion process.
Hardware fracture. Metal screws, rods, and plates used to stabilize the spine are called “hardware.” The hardware may move or break before your vertebrae are completely fused. If this occurs, a second surgery may be needed to fix or replace the hardware.
Bone graft migration. In rare cases (1 to 2%), the bone graft can move from the correct position between the vertebrae soon after surgery. This is more likely to occur if hardware (plates and screws) are not used to secure the bone graft. It’s also more likely to occur if multiple vertebral levels are fused. If this occurs, a second surgery may be necessary.
Transitional syndrome (adjacent-segment disease). This syndrome occurs when the vertebrae above or below a fusion take on extra stress. The added stress can eventually degenerate the adjacent vertebrae and cause pain.
Nerve damage or persistent pain. Any operation on the spine comes with the risk of damaging the nerves or spinal cord. Damage can cause numbness or even paralysis. However, the most common cause of persistent pain is nerve damage from the disc herniation itself. Some disc herniations may permanently damage a nerve making it unresponsive to decompressive surgery. In these cases, spinal cord stimulation or other treatments may provide relief. Be sure to go into surgery with realistic expectations about your pain. Discuss your expectations with your doctor.
Sources & links
If you have more questions, please contact the Call Us: (214) 396-3647 | (888) 373-3720
Fax #: (888)238-9155 | E-mail Us Come see on of our Doctors today please visit https://www.becomepainfree.com/
Sources
- Bose B: Anterior cervical instrumentation enhances fusion rates in multilevel reconstruction in smokers. J Spinal Disord 14:3-9, 2001.
- Hilibrand AS, et al.: Impact of smoking on the outcome of anterior cervical arthrodesis with interbody or strut-grafting. J Bone Joint Surg Am 83-A:668-73, 2001.
- Xie JC, Hurlbert RJ. Discectomy versus discectomy with fusion versus discectomy with fusion and instrumentation: a prospective randomized study. Neurosurgery 61:107-16, 2007.
Links Come see on of our Doctors today please visit https://www.becomepainfree.com/
www.spine-health.com
www.spineuniverse.com
www.knowyourback.org
Glossary
annulus (annulus fibrosis): tough fibrous outer wall of an intervertebral disc.
fusion: to join together two separate bones into one to provide stability.
osteophytes: bony overgrowths that occur from stresses on bone, also called bone spurs.
Call Us: (214) 396-3647 | (888) 373-3720
Fax #: (888)238-9155 | E-mail Us
Come see on of our Doctors today please visit https://www.becomepainfree.com/
Share this:

Minimally Invasive Surgery: Looking Ahead
Filed under: Surgery
The field of MIS owes its rate of expansion in part to growing consumer demands as news of these procedures spread through word of mouth and aggressive marketing campaigns conducted by developers.

While the procedures took approximately the same amount of time and resulted in similar amounts of blood loss, patients rated the LESS procedure as 40% less painful using the visual analog pain (VAP) comfort test.
Incidents of kidney cancer are on the rise in the United States, with more than 64,000 new cases diagnosed each year. With LESS, a single incision is used to remove tumors, compared to between four and six incisions needed for the procedure’s laparoscopic equivalent.
Endoscopic Vein Harvesting Given the OK
In a study of approximately 236,000 Medicare patients, the Duke University Medical Center found that endoscopic vein harvesting (EVH) of the saphenous vein for use as a bypass graft results in similar outcomes as traditional ankle-to-groin incisions.
Previous concerns linked EVH to narrowed grafts, however the five-year study with a three-year follow up showed no difference in mortality rates or incidents of revascularization and heart attacks.
Patients who underwent the EVH procedure experienced reduced on-site pain and swelling. They also had fewer complications and readmissions and were able to walk sooner after the procedure.
EVH requires between one and three 1-inch incisions and generally results in less tissue and muscle damage as well as reduced scarring compared to ankle to groin incisions. It is often recommended for patients with vascular issues who are at risk for leg wound complications.
In light of recent reform efforts, the health care industry is increasingly becoming an ideal environment for the continued growth and development of MIS. While procedural effectiveness is on par with many more open techniques, MIS typically results in shorter recovery periods. More efficient recovery means fewer resources are used while the patient regains his or her health, including less blood for transfusions and reduced manpower for physician follow-up sessions due to shorter hospital stays.
“The relationship of minimally invasive surgery to the health care industry is changing,” says Joe Flower, CEO of The Change Project, Inc., a health care futurist and policy specialist. “Surgery is becoming part of a larger arc of patient care designed to get and keep patients well.”
Outcomes-driven incentives may help give MIS the push it needs to expand more rapidly.
“Currently, many facilities incentivize in cost centers,” says William Taylor, M.D., co-founder of the Society for Minimally Invasive Spine Surgery and professor of neurosurgery at UCSD Medical Center in San Diego, CA. “Hospitals may incentivize less expensive open procedures because the instrumentation costs are reduced, saving money in a single cost center. However, when you consider the additional expense spent on longer recoveries, intensive care unit stays, physical therapy and blood transfusions, the slightly more expensive, yet more effective, minimally invasive procedure has the potential to reduce the overall cost for the hospital and benefit the patient.”
“We are seeing a growing population of young, active patients who want to stay active and aren’t interested in losing quality of life to conditions that can be treated through MIS,” Dr. Taylor says. “The same can be said for older groups of patients ages 65, 70 or 80 who are still active and aren’t willing to give that up.”
MIS techniques also continue to gain ground as more physicians who are trained to use them during residencies or fellowships join the workforce. For practitioners interested in developing these skills, additional training is often available remotely via teleconference.
Compared to open procedures, minimally invasive surgery (MIS) is linked to decreased risk of infection and other complications, as well as reduced blood loss in a wide variety of procedures from posterior approach total hip arthroplasty to minimally invasive aortic valve surgery.
“At this time, the 20% of spine surgery procedures being completed with MIS are more about minimal incisions, with the anatomy still in view. The next steps include introducing endoscopic or navigation systems to produce three-dimensional images on screens and revisiting the concept of even smaller incisions.” — William Taylor, M.D., co-founder of the Society for Minimally Invasive Spine Surgery and professor of neurosurgery at UCSD Medical Center in San DiegoMIS and Health Care Reform
Come see a doctor today at https://www.becomepainfree.com/
Call Us: (214) 396-3647 | (888) 373-3720
Fax #: (888)238-9155 | E-mail Us

